A study by an international team of researchers suggests that widespread use of an antibiotic to prevent liver disease is causing cross-resistance to a last-resort antibiotic for treating vancomycin-resistant Enterococcus faecium (VRE). The findings were published this week in the journal Nature.
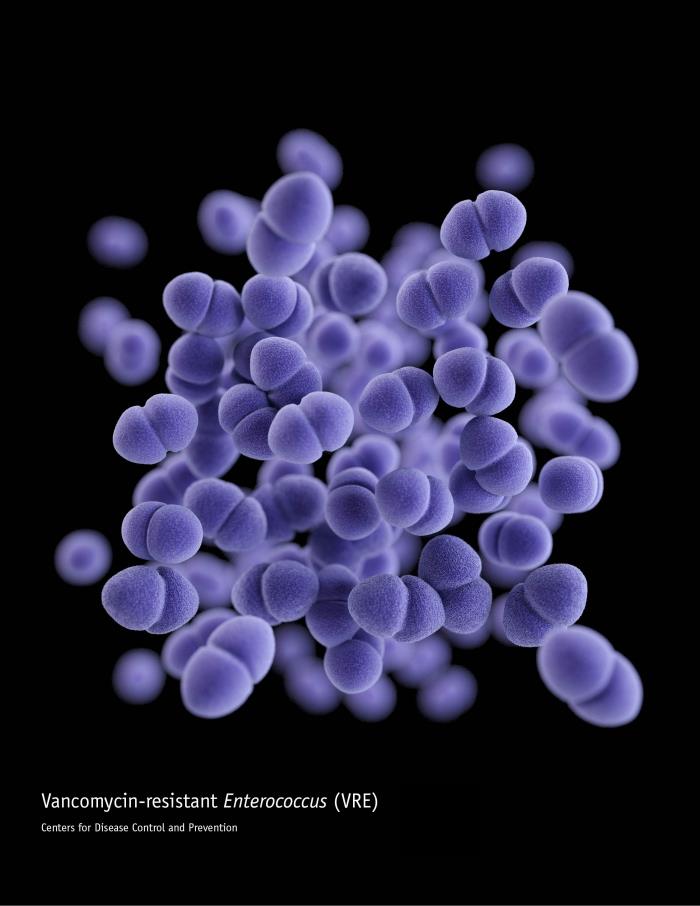
To understand the mechanisms behind increasing reports of daptomycin resistance in VRE, which is a multidrug-resistant pathogen and leading cause of hospital-related infections, a team led by researchers at the University of Melbourne conducted a combined genomic and phenotypic analysis of 998 VRE isolates collected in Australia from 2015 through 2018, 19.4% of which were daptomycin-resistant.
The analysis revealed that daptomycin resistance in VRE is caused by an amino-acid substitution (rpoB) within the bacterial RNA of VRE that's associated with the use of rifaximin, an antibiotic predominantly prescribed to prevent recurrent hepatic encephalopathy in patients with liver cirrhosis, who are frequently colonized with VRE.
Implications for VRE treatment
Further analysis showed that the emergence of the rpoB mutations coincided with the first clinical use of rifaximin in 2006, that patients with recent exposure to rifaximin were more than eight times more likely to be colonized with VRE with rpoB mutations, and that VRE isolates with rpoB mutations have spread globally. In addition, animal experiments showed that administering rifaximin to VRE-colonized mice led to the emergence of daptomycin-resistant VRE strains within the gastrointestinal tract.
"We’ve shown that rifaximin makes VRE resistant to daptomycin in a way that has not been seen before," senior author Glen Carter, PhD, of the University of Melbourne, said in a university press release. "It is also of concern that these daptomycin-resistant VRE might be transmitted to other patients in the hospital; a hypothesis that we are presently investigating."
Carter and his colleagues say the findings are surprising, since rifaximin was previously thought to be a low risk for resistance. They suggest daptomycin should be avoided for empiric therapy of VRE in patients receiving or recently treated with rifaximin, due to the higher risk of daptomycin resistance, and that rifaximin should remain a second-line option for hepatic encephalopathy prophylaxis.
We’ve shown that rifaximin makes VRE resistant to daptomycin in a way that has not been seen before.